Children’s Cancer Centre Biobank
- Project status: Active
Research area: Stem Cell Medicine > Neuro-oncology
The Children’s Cancer Centre (CCC) Biobank is a valuable collection of biological samples such as tissue collected during surgery, blood and bone marrow.
These samples are linked to health information contained in hospital medical records. Health information used may include age, gender and information about test results and medical care.
These samples are linked to health information contained in hospital medical records. Health information used may include age, gender and information about test results and medical care.
Our Biobank includes samples and health information from people with cancer, bone marrow disorders, primary immunodeficiency disease and neurofibromatosis. It also includes samples and health information from their siblings, parents and relatives.
Samples and health information in the Biobank are given to scientists in Australia and around the world. Researchers rely on these types of samples and health information to make research discoveries and medical breakthroughs. They hope to find new ways to better prevent, detect and treat different conditions.
Featured projects
Contact us
Children’s Cancer Centre Biobank
Murdoch Children's Research Institute
The Royal Children's Hospital
50 Flemington Road
Parkville VIC 3052
Australia
Louise Ludlow, CCC Biobank Coordinator
Ph:
show phone number
Email:
show email address
Information for participants
We are asking for your consent to donate your samples and use your health information for research. It is up to you whether you take part. You can say no if you want to. Your medical care will be the same regardless of whether you join the Biobank. When we say “you”, we mean you or your child.
This information will help you make an informed decision about taking part in the Biobank and will cover:
- How your samples and health information will be collected and stored.
- How your samples and health information will be used.
- How the Biobank protects your privacy and confidentiality.
- And finally, the potential risks and benefits if you decide to participate.
See our Frequently Asked Questions below for more information.
Get involved
If you would like to contribute to the Biobank, please contact us. We will give you our information statement to read and you can ask questions before you decide.
Choosing to take part in the Biobank will help researchers make a difference in medical research and to the health of future generations.
Frequently Asked Questions
Information for researchers applying for samples and health information
Step 1. Approval by the CCC Biobank Access and Oversight Committee
Initial contact by email is received from a researcher interested in obtaining samples and health information. A search of our database is undertaken to establish the approximate number of samples in storage or the feasibility of providing fresh tissue which meets requirements.
The application process is detailed to the researcher via email and our Application Form and Conditions of Use / Material Transfer Agreement forms are attached including details of partial cost recovery. Researchers must read and agree to the Conditions of Use / Material Transfer Agreement before obtaining samples and health information.
The completed application is assessed by members of the CCC Biobank Access and Oversight Committee. The committee regularly communicates electronically to accelerate the distribution of samples. Members include the CCC Biobank Coordinator, custodian of the Biobank, a pathologist and haematologist, members of the oncology team, an oncology surgeon, scientists, the clinical trials manager, a legal representative and a lay member. Samples are available to any researcher who can provide a proposal with scientific or clinical merit, Human Research Ethics Committee (HREC) approval and evidence of funding.
Applicants will be informed of the outcome of their application by email. Samples will be held for the researcher for three months from the date of approval by the Committee. If the application is denied, the committee will explain what amendments are required. Applications are accepted pending governance and ethical approval.
Step 2. Ethics and Governance approval by The Royal Children's Hospital (RCH) Human Research Ethics Committee (HREC) (if applicable)
The researcher then submits their ethics and governance application to The RCH HREC. The CCC Biobank Access and Oversight Committee approval form must be included in the application to Research Ethics and Governance.
It is the researcher’s responsibility to inform the CCC Biobank of any delays in gaining governance and ethics approval. If ethical approval has been granted from the researcher’s host institution, please forward it to the CCC Biobank Coordinator.
Step 3. Delivery of samples and progress reports
The applicant then informs the Biobank Coordinator of governance and ethics approval by providing the HREC approval certificate. The applicant is asked to forward details of their World Courier account number (or equivalent) to facilitate delivery of samples (if applicable). If the applicant is a local researcher, then arrangements are made for samples to be collected from The Royal Children's Hospital.
The researchers are required to provide a brief progress report 12 months following receipt of the samples and also a report following completion of the project. These reports should indicate the percentage of samples that have provided useful information, whether the study is continuing, and the anticipated date of study completion.
They will not be requested to reveal the results of the study in this report. A copy of all publications (peer-reviewed manuscripts and conference abstracts) resulting from the use of CCC Biobank samples should be forwarded to the Biobank upon acceptance by the conference/journal committee. This feedback is crucial to the CCC Biobank for its own applications for ongoing funding so that samples can continue to be collected, processed and stored for future applicants.
Any sample remaining following the completion of the research project must be returned to the Biobank. It will be noted in the database that the integrity of these samples is unknown and may be compromised. This information will be disclosed to researchers wanting to access these returned samples. Cell lines must not be distributed by researchers without prior approval by the Biobank Coordinator.
The CCC Biobank must be acknowledged in all publications or presentations arising from the use of samples. In the case of a collaborative investigation, recognition should be in keeping with international standards on authorship.

Image: CCC Biobank tubes
Research team
Lead researchers
Professor David Eisenstat
Director Children’s Cancer Centre, and Principal Investigator
Dr Louise Ludlow
Children’s Cancer Centre Biobank Coordinator
CCC Biobank members
Elena Fernandez
Children’s Cancer Centre Biobank Research Assistant
Kiera Williams
Children's Cancer Centre Biobank Laboratory Technician

Image: Louise Ludlow (CCC Biobank Coordinator) liaises with researchers to support their translational research projects
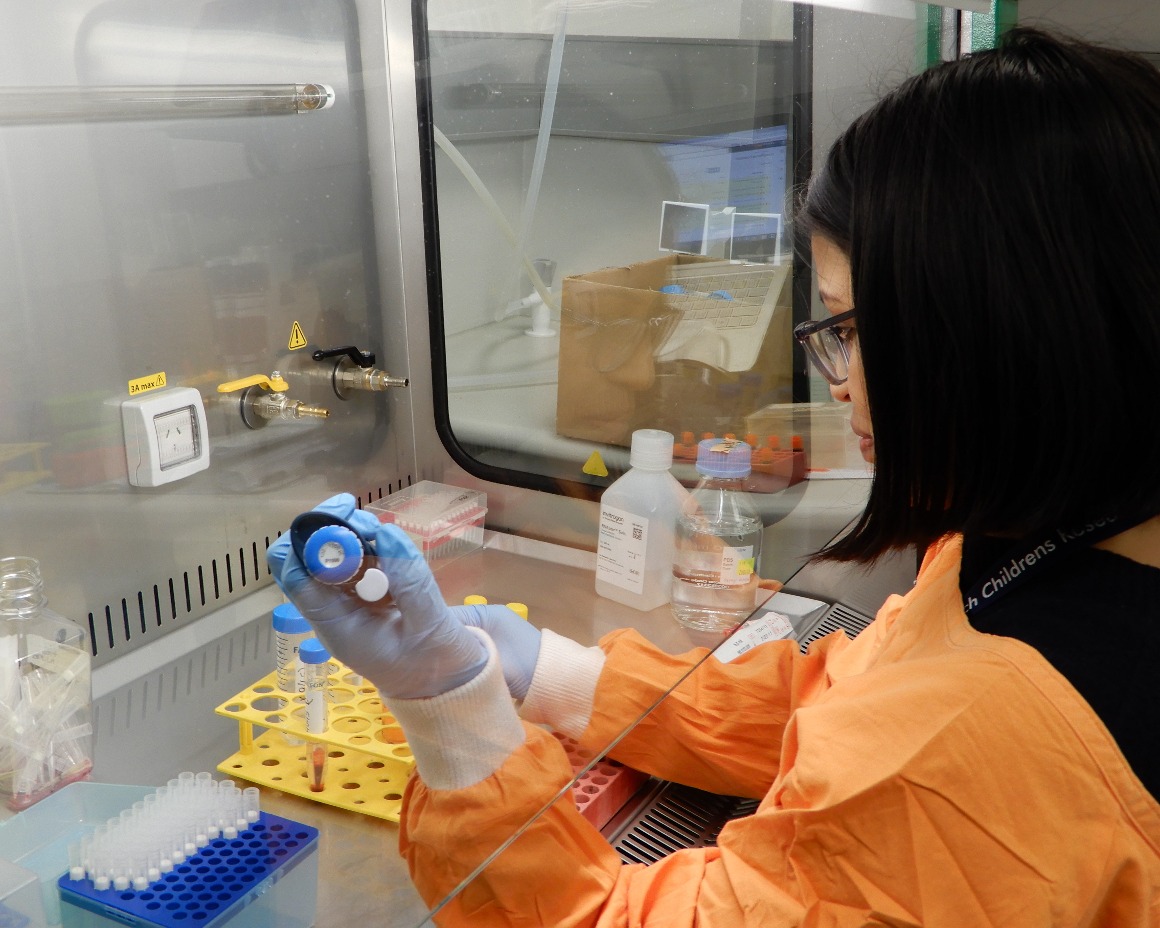
Image: Elena Fernandez (CCC Biobank Research Assistant) processing a blood sample from a patient with neuroblastoma.
CCC Biobank Access and Oversight Committee Members
Chair: Dr Nitya Phillipson
Research Quality, Governance and Integrity Lead, Office of Research, MCRI
Deputy Chair: Dr Louise Ludlow
CCC Biobank Coordinator.
Janine Campbell
Haematology, The Royal Children's Hospital (RCH)
Marty Campbell
Neuro-oncology and solid tumour stream leads, CCC, The Royal Children's Hospital (RCH)
Professor David Eisenstat
Director CCC and Group Leader, MCRI
Associate Professor Paul Ekert
Translational Tumour Biology Group Leader
Children's Cancer Institute Australia and Peter MacCallum Cancer Centre
Kahlia Fox
Clinical Trials Manager, CCC, The Royal Children's Hospital (RCH)
Associate Professor David Elliott
Team leader MCRI
Jordan Hansford
Neuro-oncology, Women’s and Children’s Hospital, Adelaide
David Hughes
Consultant Paediatric Haematologist / Oncologist, CCC, The Royal Children's Hospital (RCH)
Duncan MacGregor
Director of Anatomical Pathology, The Royal Children's Hospital (RCH)
Marion Watrin
Snr Contracts Manager, Business Development and Legal Office, MCRI
David Scanlon
Lay member and previous The Royal Children's Hospital (RCH) Human Research Ethics Committee member
Australian and New Zealand Children's Haematology/Oncology Group - Biobanking Network Funding
Major contributors
The CCC Biobank is funded by CIKA (Cancer In Kids @ RCH) and The Royal Children’s Hospital Foundation. The remainder of funds and in-kind support are provided by The Royal Children’s Hospital and Murdoch Children’s Research Institute.
Additional funding
Funds to process blood and bone marrow from patients with leukaemia were provided by the Leukaemia Auxiliary at Royal Children's Hospital (LARCH).
Funding provided by the Children’s Cancer Foundation and My Room from 2007 to 2013 for the Children's Cancer Tumour Bank supported the collection and storage of tissue samples, providing the core collection for today’s Biobank.
Collaborators
The CCC Biobank is a member of the Australian and New Zealand Children's Haematology/Oncology Group - Biobanking Network (ANZCHOG-BN).
The Children’s Cancer Centre (CCC) Biobank is also a member of Brain Cancer Biobanking Australia (BCBA).


Our research
The CCC Biobank enables translational research and supports clinical trial sample processing. Approximately 60% of participants have had one of their specimens utilised in a research project. Please find below a selection of research projects supported by the CCC Biobank.
Use of Human Tissues for the Study of Langerhans Cell Histiocytosis (LCH)
Researchers
George Kannourakis, Sharon Olsen and Jenee Mitchell from the Fiona Elsey Cancer Research Institute, Ballarat.
LCH is a rare and poorly understood disease where dendritic cells abnormally accumulate, resulting in destruction of adjacent tissues. Dendritic cells normally act as antigen-presenting cells where their main function is to process and present antigens to the T cells of the immune system.
The research project at the Fiona Elsey Cancer Research Institute in Ballarat aims to characterize the various cells within LCH lesions and blood from LCH patients, with a specific focus on these dendritic cells, T cells and T cells with a regulatory function.
This research requires cryopreserved live cells from patients with LCH that can be analysed through our flow cytometer. This research has allowed us to publish the identification of a previously unreported unusual type of T-cell in LCH and we hypothesize that further studies will show that T cells with a regulatory function are altered in LCH.
A comprehensive study of the immune response pathways in LCH will provide valuable insights into the pathogenesis of LCH.
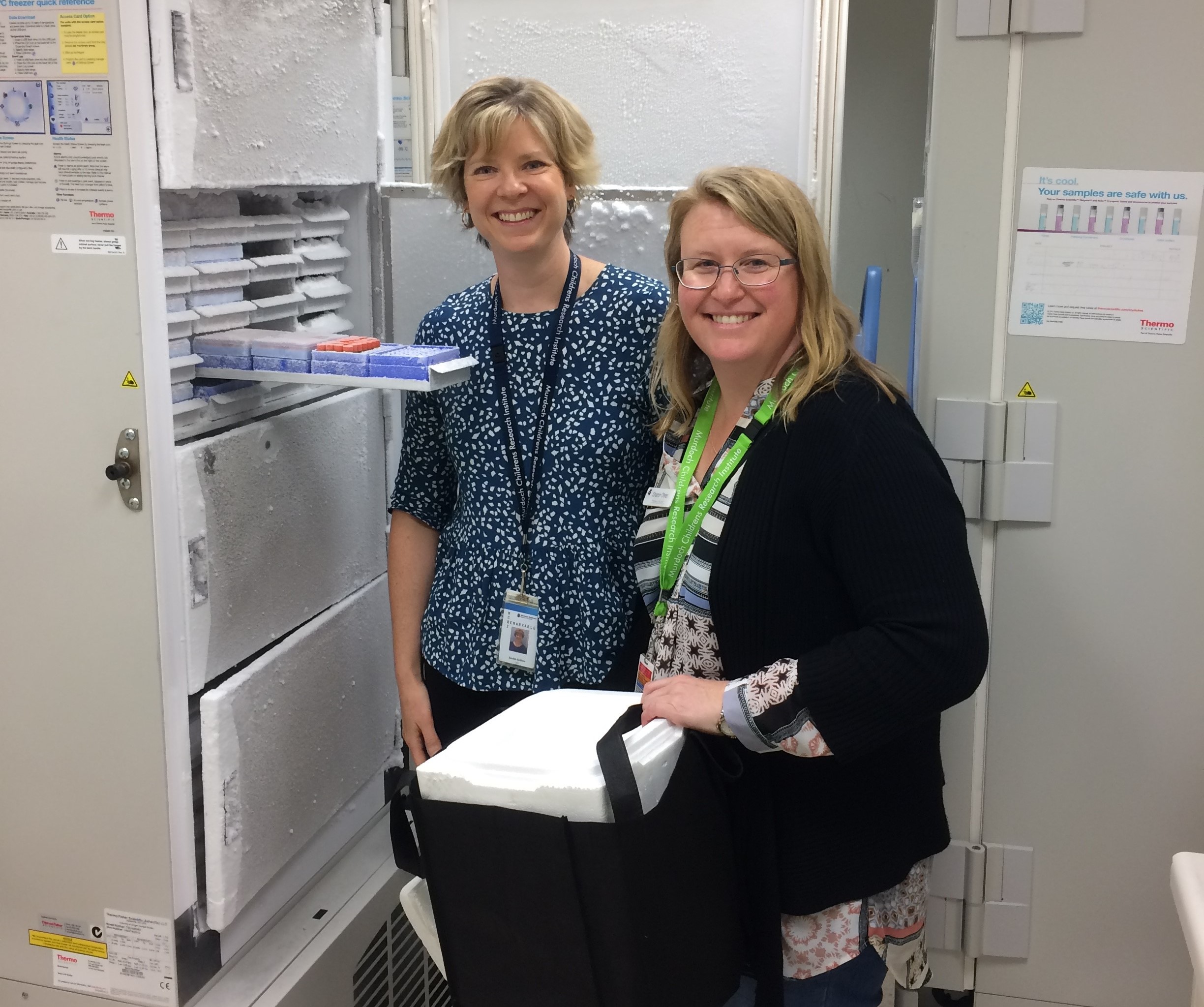
Image: In October 2016 Sharon Olsen from the Fiona Elsey Cancer Research Institute in Ballarat visited the Children’s Cancer Centre Biobank to obtain samples from Louise Ludlow (Biobank Coordinator). The use of LCH tissue samples in this project was approved by the Children's Cancer Centre Biobank Access and Oversight Committee. This project is ongoing with the most recent delivery of samples in February 2022. You can find the publication below.
Understanding the genetic basis of chemotherapy-induced heart disease
Researchers
Rachel Conyers, Dave Elliot, Lorna McLeman, Michael Cheung, Michelle Martin and Emma Masango (Murdoch Children's).
 A side effect of several valuable chemotherapeutic drugs is heart damage. Cancer survivors treated with these drugs are nine times more likely than the average, to develop heart failure. However, only 20-30% of patients are susceptible to chemotherapy-induced heart disease.
A side effect of several valuable chemotherapeutic drugs is heart damage. Cancer survivors treated with these drugs are nine times more likely than the average, to develop heart failure. However, only 20-30% of patients are susceptible to chemotherapy-induced heart disease.
Currently, there are no longitudinal studies in Australia that seek to collate all patients exposed to cardiac toxicity oncology medications. This study will aim to begin recording all patients exposed to heart-toxic medications ultimately with the aim to understand their long-term outcome, cost of health care, and interventions for cardiac complications and provide a platform for genetic studies into anthracycline cardiac toxicity.
A novel exciting approach called stem cell technology was used to create a functional assay with patient samples. This technology allowed the creation of induced pluripotent stem cell (iPSC) lines. Blood cells were reprogrammed to stem cells which were then turned into cardiomyocytes (cardiac muscle cells). The cardiomyocytes were used in functional assays to assess sensitivity to these chemotherapeutic drugs.
The goal is to set up a clinically applicable tool to predict patient sensitivity to chemotherapy. This will enable more tailored chemotherapy for patients resulting in less cardiac toxicity.
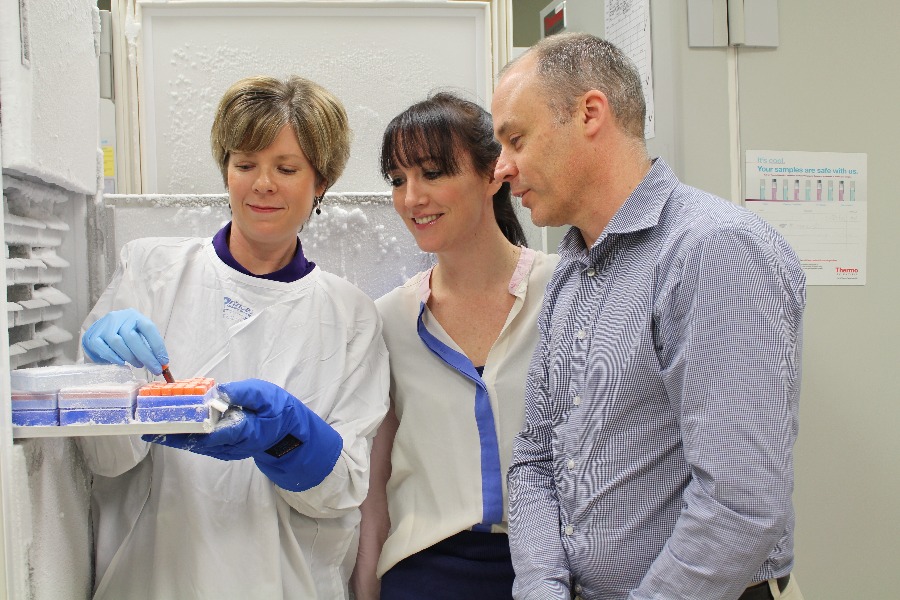
Image: Rachel Conyers and David Elliot discuss sample processing with Louise Ludlow (Biobank Coordinator). The CCC Biobank has facilitated the processing of samples towards this project since 2018.
Identification of genetic drivers in paediatric subcutaneous panniculitis-like T-cell lymphoma: an integrative clinical and genomic analysis
Researchers
Dong Anh Khuong Quang and Rachel Conyers from the Murdoch Children's Research Institute in collaboration with Prof Nada Jabado from McGill University Health Centre, Montreal, Quebec, Canada
Subcutaneous panniculitis-like T-cell lymphoma is a rare form of T-cell lymphoma. This lymphoma is most common in young adults, and although the age range is broad, it rarely affects children. Patients typically present with multiple subcutaneous lesions, which are sometimes associated with symptoms that affect the entire body and/or laboratory abnormalities such as a reduction in the number of blood cells. It has only been identified as a separate entity since 2005 and is officially included in the 2008 World Health Organization classification.
To date, less than 30 paediatric patients have been reported in the literature and mostly as individual case reports or part of a series of mostly adult patients, with limited biological data. These cases differ from their adult counterparts and there is no well-defined treatment strategy. Although cancer is often multifactorial, genetics likely plays a key role in this instance, because patients often have a common genetic background (Pacific Islanders).
The research project aims to perform DNA sequencing of tumours using next-generation technologies and to shed light on potential key genetic players in their formation. The CCC Biobank supplied tissue from two patients, contributing significantly to this multi-centric study. This will lead to an improved management strategy for these patients for which there is no standard of care.
This research project using samples from the CCC Biobank was completed and published in Nature Genetics.
Characterisation of Diffuse Midline Gliomas
Researchers
Associate Professor Misty Jenkins, Valeria Arccucci and Shiqi Stacie Wang from The Walter and Eliza Hall Institute of Medical Research
 Diffuse Midline Gliomas, otherwise known until recently as Diffuse Intrinsic Pontine Glioma (DIPG), is a paediatric brain tumour located in the brainstem and affects approximately 20 children per year in Australia with a mean age at diagnosis of 6-7 years.
Diffuse Midline Gliomas, otherwise known until recently as Diffuse Intrinsic Pontine Glioma (DIPG), is a paediatric brain tumour located in the brainstem and affects approximately 20 children per year in Australia with a mean age at diagnosis of 6-7 years.
The progression free survival has remained at 9 months for decades and sadly <10% of children are alive at two (2) years. Unfortunately, by its inherently ‘diffuse and infiltrative nature’ in an essential functional area of the brain, surgical resection of this tumour is impossible, and many different chemotherapeutic approaches for decades have been ineffective.
Radiotherapy only extends lifespan and is used as a palliative measure. Immunotherapy, an approach to use the body’s own immune system to identify and eradicate tumours, has recently been used in leukaemia and adult cancers such as melanoma and kidney tumours, with great success.
We aim to identify new targets for immunotherapy treatments, by analysis of the currently stored specimens in the CCC Biobank. By analysing the tissue for proteins expressed in DIPG, we will identify potential targets for immunotherapy treatments for DIPG. This research is essential, given there are no current curative treatments for DIPG.
Image: Misty Jenkins, Shiqi Stacie Wang and team members from The Walter and Eliza Hall Institute of Medical Research.
The identification of a novel prognostic marker in ALL
Researchers
Susie Nilsson and Ben Cao from Biomedical Manufacturing, CSIRO
 Acute lymphoblastic leukaemia (ALL) is the most common childhood cancer and although high remission rates can be achieved with standard chemotherapy, drug resistance and cancer relapse remains a significant problem. Leukaemic cell survival and drug resistance are regulated by various receptor-protein interactions that occur in the bone marrow.
Acute lymphoblastic leukaemia (ALL) is the most common childhood cancer and although high remission rates can be achieved with standard chemotherapy, drug resistance and cancer relapse remains a significant problem. Leukaemic cell survival and drug resistance are regulated by various receptor-protein interactions that occur in the bone marrow.
We have identified a specific receptor called “integrin α9β1” that we show to be expressed on a cohort of ALL samples and our preliminary results suggest the expression of this receptor is associated with drug resistance and poor prognosis.
This project seeks to validate integrin α9β1 as a prognostic marker for poor survival in paediatric ALL, which we can use to categorise patients as low or high risk as a means of directing the best course of treatment. If successful, this project will significantly change best clinical practice for the treatment of ALL in Australia.
Image: Susie Nilsson and Ben Cao from Biomedical Manufacturing, CSIRO have utilised cryopreserved bone marrow samples from 140 participants to date.
Study of retinoblastoma using transcriptomic profiling identification
Researchers
Associate Professor Raymond CB Wong, Sandra Staffieri, Sandy Hung and Alex Hewitt (Cellular Reprogramming Unit and Clinical Genetics Unit, Centre for Eye Research Australia.
 Retinoblastoma is the most common eye cancer in children, causing blindness or, in some cases loss of the affected eye. Despite intensive research efforts, currently, it is unclear which cell types within the retina give rise to retinoblastoma. A better understanding of this would allow us to target the right cells and develop new treatments for retinoblastoma with better outcomes.
Retinoblastoma is the most common eye cancer in children, causing blindness or, in some cases loss of the affected eye. Despite intensive research efforts, currently, it is unclear which cell types within the retina give rise to retinoblastoma. A better understanding of this would allow us to target the right cells and develop new treatments for retinoblastoma with better outcomes.
This project aims to utilise transcriptomics to survey retinoblastoma tumours from patients in high resolution. This allows us to build a detailed gene map for the human retina and examine how the genetic signals are deregulated and how retinal cells are affected in retinoblastoma.
Our findings will help identify the retinal cell types that give rise to retinoblastoma, and potentially discover gene markers that could develop new drug treatments and diagnostic tests.
Image: Dr Raymond Wong (Centre for Eye Research Australia)
Single cell RNA-seq sequencing of paediatric low-grade gliomas
Researchers
Pratiti Bandopadhayay, Rameen Beroukhim and Alexandra Condurat (Dana Farber Cancer Institute, Boston).
Cancer is thought to be primarily a disease that results from the acquisition of a sequence or combination of somatic genetic alterations. Such genetic alterations generally disturb the function of two classes of genes, tumour suppressor genes and oncogenes. In the latter, somatic mutation results in the loss of function of the gene product, whereas in the former, somatic mutations lead to a gain of function.
A description of these mutations, and how these mutations co-segregate in cancers with varying etiology and response to treatment, will likely enable improved classification that properly represents the variability of these cancers. It will also be likely to lead to an improved understanding of their underlying biology, potentially leading to the identification of new therapeutic targets.
This research team are characterising the cellular programs of individual low grade glioma cells to determine how they grow.
Towards improving MPNST molecular diagnosis for patients with neurofibromatosis type 1 through a liquid biopsy test
Researchers
Smadar Kahana-Edwin and Jonathan Karpelowsky (Children’s Cancer Research Unit, Kids Research, The Children’s Hospital at Westmead).
 Different cells and tissues, including solid cancers, shed biomaterial into the blood. Liquid biopsy is a novel method to detect such biomolecules and its clinical utility is being investigated for diagnosis of different diseases and conditions, including early cancer detection.
Different cells and tissues, including solid cancers, shed biomaterial into the blood. Liquid biopsy is a novel method to detect such biomolecules and its clinical utility is being investigated for diagnosis of different diseases and conditions, including early cancer detection.
For many years, the suboptimal sensitivity of circulating cancer biomarker assays delayed future progress in this field. Recent technological developments have changed that, pushing liquid biopsy into the clinic.
Accurate malignant peripheral nerve sheath tumour (MPNST) diagnosis poses a challenge in current clinical settings. For patients with NF1, where multiple plexiform neurofibroma (pNF) lesions may develop throughout their lifetime, each can potentially lead to MPNST, this challenge is even greater.
The Liquid Biopsy Research Group at the Children’s Hospital at Westmead (NSW), aims at filling this significant gap. Molecularly, pNF and MPNST have different DNA signatures. Here, we propose to explore whether these signatures can be detected in the blood of NF1 patients having pNF and MPNST, in order to aid an accurate diagnosis of MPNST, using a simple blood test.
Image: Smadar Kahana-Edwin and Jonathan Karpelowsky from the Children’s Cancer Research Unit, Kids Research, The Children’s Hospital at Westmeade.
Investigating the cellular and molecular biology of oncogenes and translocations
Researchers
A/Prof Paul Ekert (Translational Tumour Biology Group Leader, Children's Cancer Institute Australia and Peter MacCallum Cancer Centre and MCRI)
Cancer is a disease caused by changes in the genes specifically within the cancer cells. A variety of such changes are recognized for example, there are changes in which the code of the gene is altered (mutations). Of particular interest in cancer are changes where parts of two genes that are normally separate are fused to form a new gene with new properties that drive the development of the cancer.
This study focuses on the basic biology of how these gene changes function to produce cancer and the way in which they are identified in patients.
Testing sensitivity of cancer cells to new drugs
Researcher:
Christine Hawkins (Biochemistry and Genetics, La Trobe University)
Cure rates for some types of cancers such as osteosarcoma and Ewings sarcoma remain low. We hope that recently developed anti-cancer drugs that work via different molecular mechanisms to chemotherapy, may be effective treatments for some of these cancer types.
We will test the ability of these new drugs (or combinations of drugs) to kill cells isolated from paediatric patients' tumours in the laboratory, to predict the utility of each drug for each kind of cancer. The cancer cells will be obtained from The Children’s Cancer Centre Biobank.
Translocation of ER Chaperones to the Cell surface in Paediatric Glioblastoma Multiforme
Researchers
Dr Angelica Merlot and Alexis Minchaca (Cancer Targets and Therapeutics Team in the Tumour Biology and Targeting Group, Children’s Cancer Institute Australia)
Glioblastoma is a highly aggressive tumour with a poor prognosis for adult and paediatric patients. There is an urgent need for the identification of new therapeutic targets. Endoplasmic reticulum (ER) chaperones have been shown to be translocated to the cell surface during cancer state, promoting tumour survival. Importantly, they are selectively expressed in cancer compared to normal tissues. Additionally, their pro-tumoural function is cancer and cell type specific. However, the surface expression of ER chaperones in glioblastoma has not been investigated in adult or paediatric populations.
We aim to assess the surface localisation of ER chaperones in GBM patient tissue samples and primary cultures.
Mutational Landscape of Juvenile Granulosa Cell Tumours
Researchers
Dr Simon Chu (Hormone Cancer Therapeutics Laboratory, Hudson Institute of Medical Research) and Peter Fuller (Centre for Endocrinology and Metabolism, Hudson Institute of Medical Research).
Granulosa cell tumours (GCT) of the ovary arise from the granulosa cells in the ovary; they are a unique subset of ovarian cancers which do not respond to conventional therapy for ovarian cancer. There are two forms of this disease, known as either adult GCT or juvenile GCT. The juvenile subtype, defined by both age of onset and histology, represents about 5% of GCT. Mutations that cause this disease are currently unknown.
These studies will identify the genetic mutations that either drive the disease, or lead to aggressive and/or advanced disease, which has a mortality of ~80% in affected girls/women. The studies will examine genes which we have found to be over expressed in advanced disease and therefore may contribute to the progression of the disease; blocking these may provide novel treatment options. The identification of tumour specific mutations may also provide specific approaches to treatment, such as personalised medicine for girls/women with GCT.
Cancer newsroom
Immunocompromised Infections

Pioneering safer radiotherapy for children with cancer

Safeguarding children undergoing cancer treatments

Protecting children receiving cancer treatment from infections

Dr Sohinee Sarkar receives Strategic Research Fund Fellowship

AUS-POND: Australian Paediatric Pharmacogenetics Oncology Network for Drug Safety

NHMRC Ideas Grants to advance childhood treatments and diagnoses

Prof Kathryn North AC delivers inaugural keynote address for Marie Krogh Prize

Alleviating the cruel toll of cancer treatment

Pioneering project to provide safer childhood cancer treatments

Share //

